Award-winning PDF software





Disclosure of ownership bcbs Form: What You Should Know
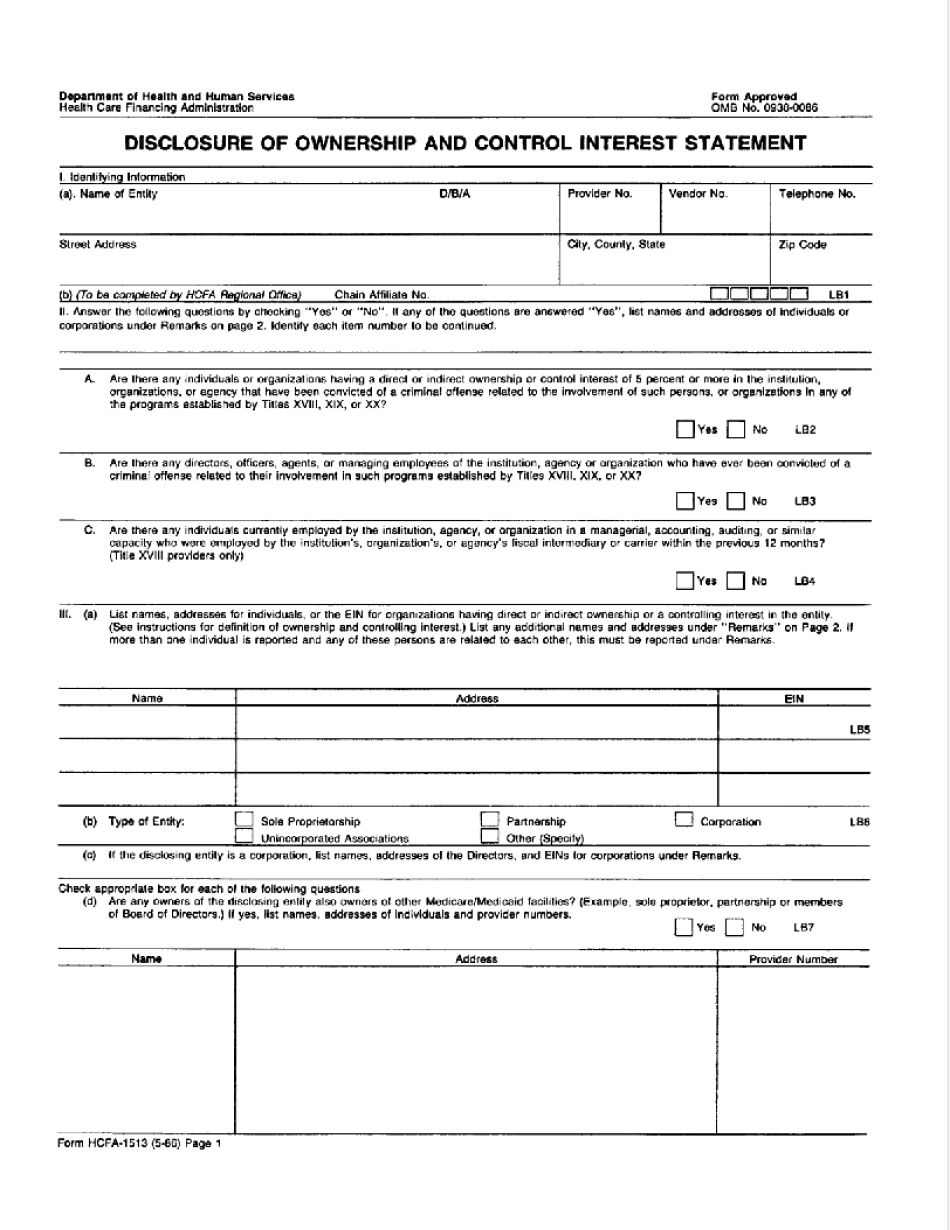
SUBJECT: Provider Disclosure of Ownership and Control Statement/Determination The providers below disclose ownership or control of any individual or entity as follows: (A) A medical supplier, (B) A provider of medical/surgical supplies and equipment, (C) A professional health service/benefits provider for individuals with disabilities, (D) A provider of medical/surgical supplies and equipment that provides health care to individuals with psychiatric disabilities, (E) A provider of medical/surgical supplies and equipment that provides health care to individuals with drug/alcohol use disorders, (F) A provider of medical/surgical supplies and equipment that provides health care to individuals with trauma, (G) A provider that is not employed by the provider's employer, (H) An independent contractor of the above providers or the provider's employers (I) A provider of medical/surgical supplies and equipment that offers health care to individuals with other disorders, and (J) A medical or surgical supplier. No individual or entity that is not a healthcare provider may disclose the identity of their specific employees. Disclosure of Ownership and Control Letter: If not a person or business, please identify the individual or entity that has control over this provider's activities. (See enclosed letter.) List any other individuals with a direct or indirect interest in the provider or supplier's activities. If the provider is a person, please identify the person's name, role and contact information. (D) list any other persons who control or are involved in the provider's activities; or (E) list the nature of the relationship or involvement between the provider and the person listed in (I-J). List the names of all individuals with whom you have communicated with regarding this listing, their contact information (phone # and email) and any relationship of any kind between you and such individuals. (F) For each individual you have been in contact with about this listing, list the following; (e) Name and location of their provider. (f) Name of their employer. You also will need to include, in all letters, a list of all contracts between this provider and any entity, partnership, joint venture, limited liability partnership, or other entity which the provider has a contractual relationship with. These can include any organization, including, if applicable, a federal, state, or local government.
online solutions help you to manage your record administration along with raise the efficiency of the workflows. Stick to the fast guide to do HCFa-1513, steer clear of blunders along with furnish it in a timely manner:
How to complete any HCFa-1513 online: - On the site with all the document, click on Begin immediately along with complete for the editor.
- Use your indications to submit established track record areas.
- Add your own info and speak to data.
- Make sure that you enter correct details and numbers throughout suitable areas.
- Very carefully confirm the content of the form as well as grammar along with punctuational.
- Navigate to Support area when you have questions or perhaps handle our assistance team.
- Place an electronic digital unique in your HCFa-1513 by using Sign Device.
- After the form is fully gone, media Completed.
- Deliver the particular prepared document by way of electronic mail or facsimile, art print it out or perhaps reduce the gadget.
PDF editor permits you to help make changes to your HCFa-1513 from the internet connected gadget, personalize it based on your requirements, indicator this in electronic format and also disperse differently.