Music: This Medicaid provider agreement is a contract between you (the Ohio Department of Medicaid). - To read all parts of the agreement, make sure to scroll all the way down. - You will have the opportunity to print the agreement if you desire. - The agreement requires your electronic signature. - Type your name into the text exactly as you entered it on the demographics tab. - It must match exactly. - If you entered a middle initial, you must type a middle initial with no punctuation. - If it doesn't match, you'll receive an error. - Click "agree" and then click "Save and continue." - Music.
Award-winning PDF software





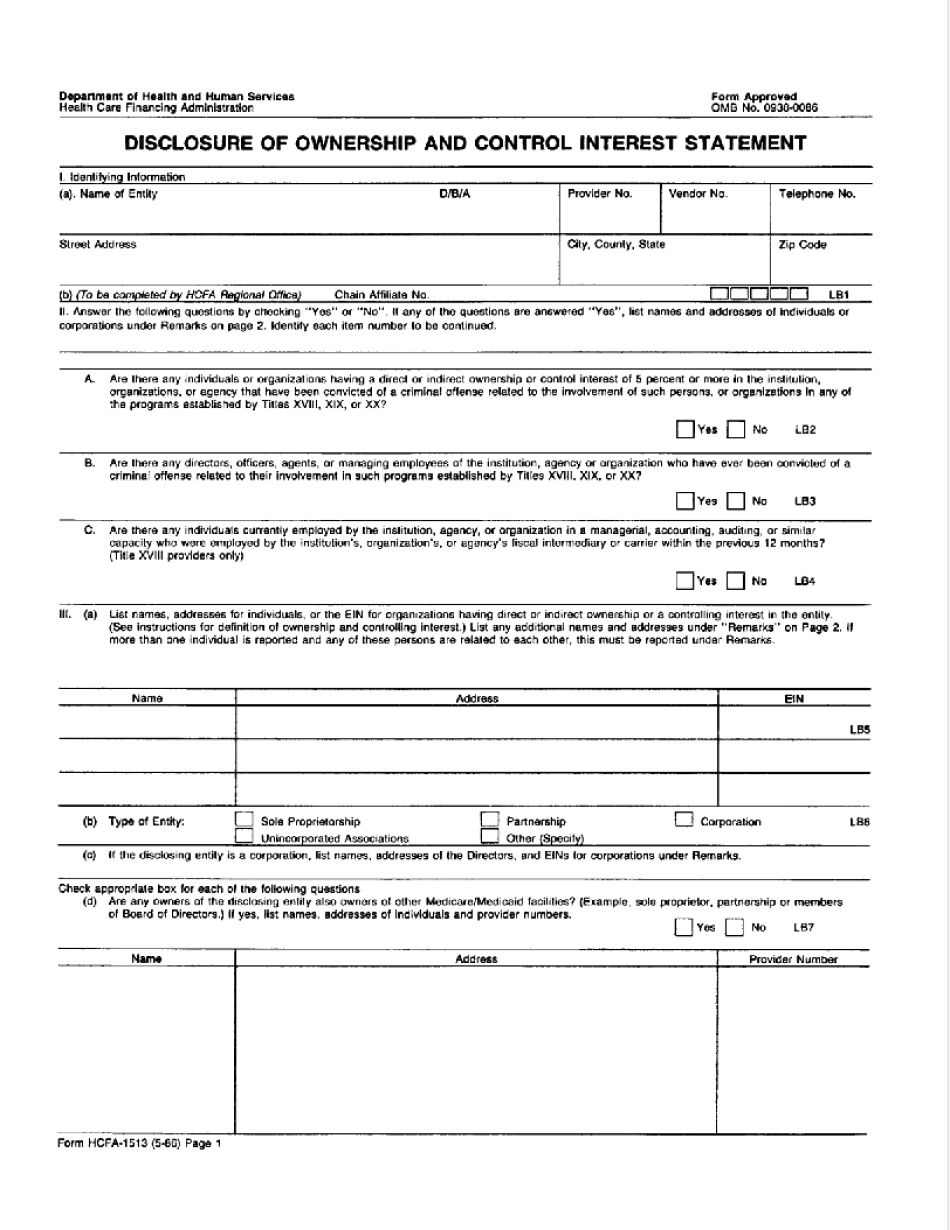
Medicaid provider disclosure requirements Form: What You Should Know
Information shall constitute an Acknowledgment of Information Failure and a penalty will be imposed. E-Mail Submission of this Form to: Patient Information (Alabama Medical Home) Submit by e-mail to: info medicare.Alabama.gov The completed form may only be filled out by the recipient. No faxes will be accepted. A copy of the completed form may be faxed to the following: Medicaid Disclosure Form — New Mexico Medicaid Forms need to be filled out, notarized, and forwarded to PHS to process. This form can be used to update a group or other Medicaid entity registration or to amend any of the information supplied on the previous form, but no other changes are permitted. E-Mail Submission of this Form to: Patient Information (Alabama Medical Home) Submission of this form is required to establish a new group or payee or update an existing group or payee. This form may be amended by anyone who has, before the date it is submitted, received written notification from the administrator of the group or payee that the previous forms have not been properly completed (i.e. by the physician who signed the previous forms). No changes are permitted, other than those approved by the administrator of the group or payee. The information provided in the previous forms must be used exactly as it was originally provided in the form they are updated on. Please use the form provided and follow the directions in the e-mail you receive to complete the form. No changes are permissible. No faxes are accepted. A copy of the completed form may be faxed to the following: The completed form may only be filled out by the recipient. No faxes are accepted.
online solutions help you to manage your record administration along with raise the efficiency of the workflows. Stick to the fast guide to do HCFa-1513, steer clear of blunders along with furnish it in a timely manner:
How to complete any HCFa-1513 online: - On the site with all the document, click on Begin immediately along with complete for the editor.
- Use your indications to submit established track record areas.
- Add your own info and speak to data.
- Make sure that you enter correct details and numbers throughout suitable areas.
- Very carefully confirm the content of the form as well as grammar along with punctuational.
- Navigate to Support area when you have questions or perhaps handle our assistance team.
- Place an electronic digital unique in your HCFa-1513 by using Sign Device.
- After the form is fully gone, media Completed.
- Deliver the particular prepared document by way of electronic mail or facsimile, art print it out or perhaps reduce the gadget.
PDF editor permits you to help make changes to your HCFa-1513 from the internet connected gadget, personalize it based on your requirements, indicator this in electronic format and also disperse differently.
Video instructions and help with filling out and completing Medicaid provider disclosure requirements
